Case Study — When “Just Tripping” Isn’t So Simple: Understanding EPM
A 14-year-old Warmblood gelding, actively competing as hunter, was presented with a subtle but concerning change: intermittent tripping under saddle.
Initially, the signs were subtle. The horse remained bright, eating well, and appeared sound at the walk and trot in straight lines. However, under saddle, particularly during collected work, he began to stumble behind and occasionally felt uncoordinated to the rider.
Clinical Findings
On examination, several mild neurologic deficits were identified:
Subtle hindlimb incoordination (ataxia), more noticeable on circles
Delayed protraction in the hind limbs
Mild weakness when asked to back or during tail pull
No cranial nerve deficits
Muscle loss on right side of hindquarters
Importantly, there were no signs of lameness, and flexion tests were unremarkable, raising suspicion for a neurologic, rather than orthopedic, issue.
Differential Diagnoses Considered
Cervical vertebral stenotic myelopathy (neck arthritis/wobblers)
Sacroiliac dysfunction
Equine protozoal myeloencephalitis (EPM)
Other neurologic diseases (e.g., viral)
Given the asymmetry and subtle progression, EPM was high on the list.
Diagnostic Approach: Blood Test vs. CSF Tap
One of the most common questions from owners is:
“Can we just run a blood test?”
Blood Testing (Serum Antibodies)
A blood test looks for antibodies to Sarcocystis neurona (the primary organism causing EPM).
Pros:
Easy and non-invasive
Useful as a screening tool
Helps determine exposure
Cons:
Many horses in endemic areas are seropositive but not clinically affected
A positive result does NOT confirm EPM
Cannot distinguish between past exposure and active disease
In this case, the horse returned positive on serum testing
CSF Tap (Spinal Fluid Analysis)
A cerebrospinal fluid (CSF) tap allows us to compare antibody levels between blood and spinal fluid.
Pros:
Gold standard for diagnosis
Helps confirm whether the organism has crossed into the central nervous system
Improves diagnostic accuracy significantly
Cons:
More invasive (performed under sedation)
Slight risk (rare complications)
Higher cost
IIn this case, CSF analysis showed a high antibody ratio consistent with active EPM infection, confirming the diagnosis.
Treatment and Outcome
The horse was started on a standard course of antiprotozoal therapy along with anti-inflammatories and supportive care.
Over the following weeks:
Tripping episodes decreased
Coordination improved
Returned gradually to work
Early intervention was key to a favorable outcome.
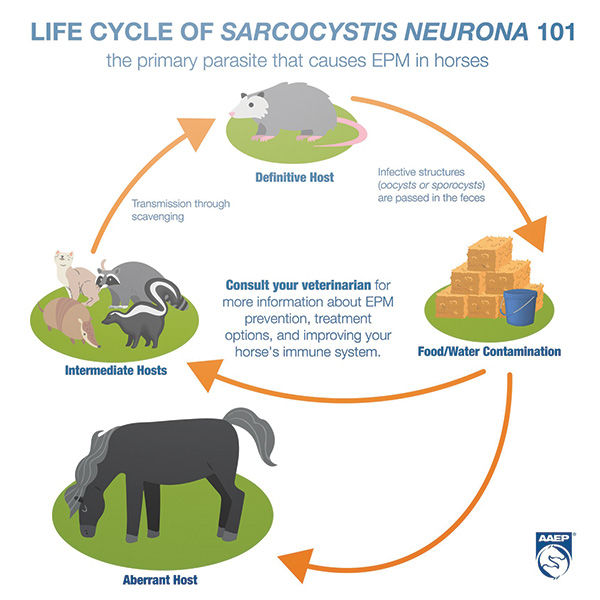
What Causes EPM?
Equine Protozoal Myeloencephalitis (EPM) is caused by microscopic parasites, most commonly Sarcocystis neurona(and less commonly Neospora hughesi), that affect the horse’s central nervous system.
The Key Player: The Opossum
The parasite’s life cycle involves the Virginia opossum, which is the definitive host. Opossums shed infective sporocysts (parasite eggs) in their feces.
How Horses Become Infected
Horses are accidental hosts, meaning they are not part of the normal life cycle.They become infected by:Eating feed or hay contaminated with opossum fecesDrinking contaminated waterGrazing in areas where opossums have accessOnce ingested, the parasite can:Enter the bloodstreamMigrate to the brain and spinal cordCause inflammation and damage to the nervous system
EPM is NOT contagious, horses cannot spread it to each otherMany horses are exposed, but only a small percentage develop diseaseThe difference often comes down to the horse’s immune system
Risk Factors
Stress (transport, competition, illness)Immune suppressionHigh wildlife exposure (barns with opossum activity)
Practical Prevention Tips
Store feed in sealed containersClean up spilled grain promptlyLimit wildlife access to barns and hay storageAvoid feeding on the ground in high-risk areas
Take-Home Messages for Owners
Subtle performance issues, like tripping or difficulty with collection, can be early neurologic signs
A positive blood test alone does not diagnose EPM but can be helpful in ruling out the disease
A CSF tap provides much more definitive information when neurologic disease is suspected
Early diagnosis and treatment significantly improve prognosis